Dental Low Plan
You pay a higher percentage for services than the High Plan
Katy ISD offers two dental plans. While both pay 100% of the cost for preventive care, the plans differ in coverages depending on the services you need and the dentist you see.
*New this year: these plans have both in and out of network coverages. Also, both plans have a maximum yearly benefit of $1,000.
Aflac Dental frequently asked questions can be found here.

You pay a higher percentage for services than the High Plan
Dental Low Plan
Low Plan
There are no copays on this plan. You’ll pay a deductible for both basic and major services. Both of these services are then covered at a percentage of the cost. There is no coverage for orthodontia on this plan. You can visit any dentist you choose, but using an in-network dentist can save you money. Remember, you have a maximum yearly benefit of $1,000.
![]()
Get started with our refreshed Member Portal or Scan the QR code.
Aflac Member Portal registration instructions help.
You can use any dentist you choose; however, your costs are lower if you use an in-network dentist. If you’d like to find an in-network dentist prior to enrolling in this plan, visit Aflac providers list or call Aflac's KISD dedicated Dental line at 877-675-7277, Monday – Friday: 8AM – 8PM (ET).
![]()
Click here to search for providers.
Have Questions? Call Aflac's KISD dedicated Dental line at 877-675-7277, Monday – Friday: 8AM – 8PM (ET) or visit the Dental FAQs.
Aflac Member Portal USER GUIDE
| Rates per pay period | |
|---|---|
| Based on 24 pay periods | |
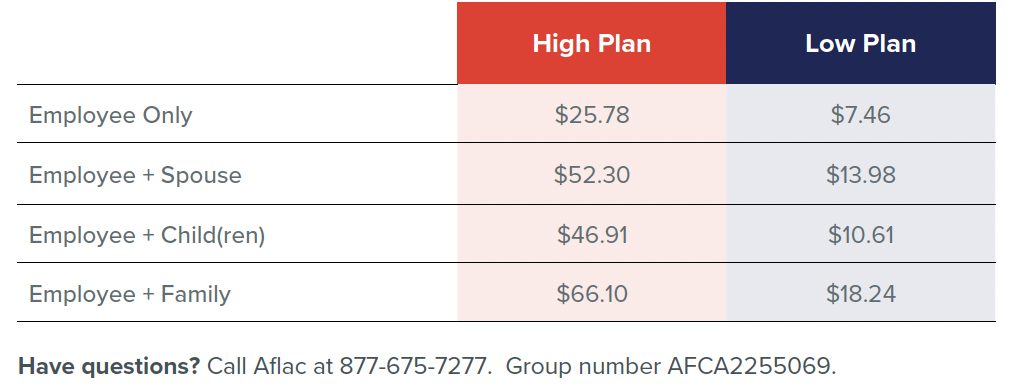
| Employee | $7.46 |
| Employee + Spouse | $13.98 |
| Employee + Child(ren) | $10.61 |
| Employee + Family | $18.24 |
| Annual deductible | |
|---|---|
| Individual | $25.00 |
| Family | $75.00 |
| Annual benefit maximum | |
|---|---|
$1,000 |
|
| Covered services | You pay |
|---|---|
| check Preventive | Covered at 100% |
Freedom to see any dentist, but using an in-network dentist can save you money.
Dental High Plan
You’ll pay a deductible for basic, major, and orthodontic care. You can visit any dentist you choose, but using an in-network dentist can save you money.
High Plan
You’ll pay a deductible for basic, major, and orthodontic care. You can visit any dentist you choose, but using an in-network dentist can save you money.
Remember, you have a maximum yearly benefit of $1,000.
![]()
You’ll pay a deductible for basic, major, and orthodontic care. You can visit any dentist you choose, but using an in-network dentist can save you money. Remember, you have a maximum yearly benefit of $1,000.
Get started with our refreshed Member Portal or Scan the QR code.
Aflac Member Portal registration instructions.
You can use any dentist you choose; however, your costs are lower if you use an in-network dentist. If you’d like to find an in-network dentist prior to enrolling in this plan, visit Aflac providers list or call Aflac's KISD dedicated Dental line at 877-675-7277, Monday – Friday: 8AM – 8PM (ET).
![]()
Click here to search for providers
Aflac Dental & Vision Insurance frequently asked questions can be found here.
Aflac Member Portal USER GUIDE
Have questions? Call Aflac's KISD dedicated Dental line at 877-675-7277, Monday – Friday: 8AM – 8PM (ET).
| Rates per pay period | |
|---|---|
| Employee | $25.78 |
| Employee + Spouse | $52.30 |
| Employee + Child(ren) | $46.91 |
| Employee + Family | $66.10 |
| Annual deductible | |
|---|---|
| Individual | $50 |
| Family | $150 |
| Annual benefit maximum | |
|---|---|
$1,000 |
|
| Covered services | You pay |
|---|
| Dental Low Plan | Dental High Plan | |||
|---|---|---|---|---|
| Rates per pay period | ||||
| $7.46 | $25.78 | |||
| Annual deductible | ||||
|
Individual $25.00 Family $75.00 |
Individual $50 Family $150 |
|||
| Annual benefit maximum | ||||
$1,000 |
$1,000 |
|||
| Covered services | ||||